Everything You Should Know About Diltiazem (Cardizem)
Diltiazem (Cardizem) is a calcium channel blocker used to slow heart rate, most commonly in conditions like atrial fibrillation with rapid ventricular response (RVR) and other supraventricular tachycardias. Understanding when to administer diltiazem, and when immediate cardioversion is required, is a critical skill taught in advanced cardiac emergency training, including ACLS certification courses . It is typically used in hemodynamically stable patients, while unstable patients require immediate electrical cardioversion.
In this guide, we'll break down when and how diltiazem is used, including its mechanism of action, dosing, guideline-supported indications, and key safety considerations for healthcare providers.
Table of Contents
- Case Presentation - Palpitations and Atrial Fibrillation with RVR
- Initial Vital Signs and Clinical Assessment
- ECG Findings – Atrial Fibrillation with Rapid Ventricular Response
- Initial Treatment with Diltiazem and Digoxin
- Post-Treatment Rhythm Conversion and Clinical Improvement
- What is Diltiazem (Cardizem)?
- Calcium Channel Blockers Overview
- Dihydropyridine Calcium Channel Blockers
- Non-Dihydropyridine Calcium Channel Blockers
- Vaughan-Williams Antiarrhythmic Classification System
- Indications for Diltiazem Use
- Mechanism of Action of Diltiazem
- When Diltiazem Should Be Avoided
- Diltiazem Use in Heart Failure and Hypotension
- Dosing and Administration of Diltiazem
- When Electrical Cardioversion is Required
- Key Clinical Takeaways for Emergency Providers
Case Presentation - Palpitations and Atrial Fibrillation with RVR
A 50-year-old male with a history of hypertension (HTN) and atrial fibrillation (AF) presents to the Emergency Department complaining of palpitations which started while mowing the lawn.
In the case of an atrial fibrillation or flutter with RVR, what should the provider look at first? The answer is hemodynamic stability and the absence of hypoperfusion. This is critical because treatment will change depending on the patient’s stability; for stable patients, treatment with diltiazem is preferred; for unstable patients, electrical cardioversion is necessary.
Initial Vital Signs and Clinical Assessment
The nurse examining the patient finds that he is alert and oriented with a Glasgow Coma Scale (GCS) of 15 and no signs of hypoperfusion. His vitals are as follows:
- Heart Rate: 165/min, strong and irregular
- Blood Pressure: 140/100 mmHg
- Ventilatory Rate: 22/min
- SpO2: 98% on room air
The patient is compliant with his medications and denies any allergies.
While not totally reassuring, it is significant that the patient’s blood pressure is stable despite the tachycardia, as this means that the left ventricle still has an adequate stroke volume despite the decreased filling time and likely loss of the atrial kick from the history of atrial fibrillation . Additionally, adequate oxygenation and mental status are required to define a patient’s status as “stable”, as is the case here. Since the patient meets these criteria, this means that diltiazem is a reasonable and preferred option of treatment.
As an aside, what would it mean if the patient was hemodynamically unstable or had signs of inadequate oxygenation? Diltiazem would cause further harm to the patient in such a scenario since the rapid heart rate is the body’s attempt to compensate for decreased cardiac or systemic perfusion. If diltiazem were given to a patient that was “toeing the line”, decreasing their heart rate and dropping their blood pressure would send them into a decompensated shock state.
ECG Findings – Atrial Fibrillation with Rapid Ventricular Response
Next for our patient, a 12-lead ECG is recorded.
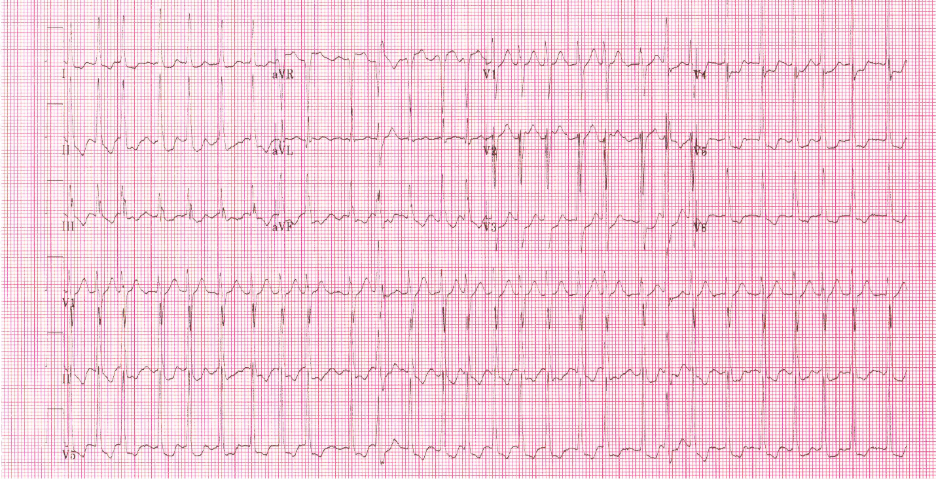
Atrial fibrillation with rapid ventricular response (RVR) and generalized ST-segment depression indicative of subendocardial ischemia.
This is a concerning finding. ST-segment changes have occurred potentially because of ischemia from an excessively rapid heart rate. While in other scenarios we may suspect coronary blockage, here we can infer that the ST depression is likely “demand ischemia” brought about by the coronary arteries receiving suboptimal perfusion during an abbreviated diastolic phase of the cardiac cycle. The blood supply is being artificially cut off from the demand of the cardiac muscle. Thus, rate control with diltiazem would likely be beneficial in providing a longer diastolic phase with increased coronary blood flow and myocardial perfusion, solving the ST depression seen above.
Initial Treatment with Diltiazem and Digoxin
The patient is treated with 20 mg of IV diltiazem over 2 min, followed by 10 mg IV over 1 hr, plus 0.25 mg IV digoxin (Lanoxin) over 3 min.
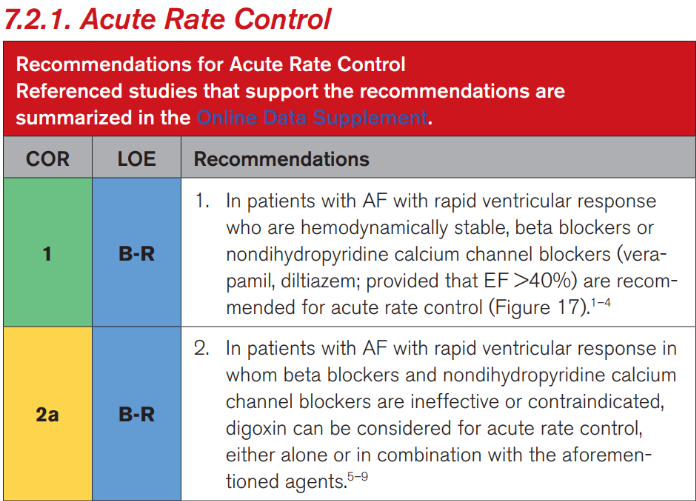
The most recent guidelines from the American College of Cardiology and the American Heart Association (2023) state that, for patients with stable atrial fibrillation with RVR, the above course of action is reasonable. In fact, the diltiazem bolus may be repeated at a slightly higher dose a second time (0.35mg/kg) if the first (0.25mg/kg) is not effective; either way, this is followed by a 5 to 15 mg/hr continuous infusion of diltiazem. A concurrent bolus of Digoxin is also reasonable, according to the guidelines, with the dosage range being 0.25 to 0.5 mg over several minutes, repeated every 6 hours for a max of 1.5mg in 24 hours. Digoxin is supported in combination with diltiazem as studies have shown a more rapid and durable response when the drugs are given in combination.
While the administration of diltiazem and digoxin is safer in hemodynamically stable patients experiencing atrial fibrillation with RVR and SVT, vital sign monitoring is critical during the hour-plus that it takes to complete the administration of these drugs since the patient’s cardiac compensatory mechanisms can still take a turn for the worse, requiring the administration to be stopped and supportive measures to be taken (digoxin immune fab, intravenous calcium, etc.).
Post-Treatment Rhythm Conversion and Clinical Improvement
Following administrations of diltiazem and digoxin, a rhythm change is noted on the monitor and another 12-lead ECG is recorded.
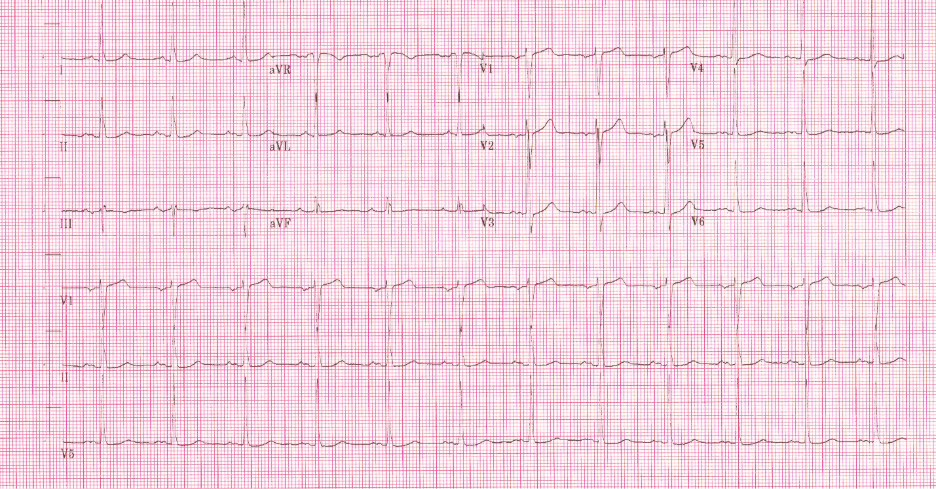
There is a sinus rhythm with left ventricular hypertrophy by limb lead voltage criteria and left atrial enlargement. There are no signs of subendocardial ischemia, suggesting the ST-segment depression was rate-related.
At this point, the patient is asymptomatic and admitted for observation without further incident.
Once rate control has been achieved, a repeat EKG is necessary to determine whether ischemia and the correlating ST depression have been resolved. If it hasn’t, we need to investigate Acute Coronary Syndrome as a probable cause instead of demand ischemia. Additionally, the controlled rhythm must be clearly defined, whether atrial fibrillation or atrial flutter, and the rhythm mist best assess for aberrations such as QT prolongation and AV block which would require adjustments in treatment.
What is Diltiazem (Cardizem)?
Diltiazem (Cardizem) belongs to the Class IV group of antiarrhythmic medications , specifically categorized as a non-dihydropyridine calcium channel blocker (non-DHP CCB) It is one of the most common pharmacological agents used for treatment of tachyarrhythmias such atrial fibrillation with RVR.
Calcium Channel Blockers Overview
Calcium channel blockers inhibit intracellular calcium influx by binding to L-type voltage-gated calcium channels in both cardiac and vascular smooth muscle cells. This reduces blood pressure and decreases the speed of AV nodal conduction, the latter of which is helpful in the management of supraventricular arrhythmias like AF with RVR.
CCB’s are further divided into two major categories with differing molecular makeup and mechanism of action – dihydropyridines and non-dihydropyridines.
Dihydropyridine Calcium Channel Blockers
Dihydropyridines (DHPs) are easily identified by the last four letters of the generic name ending with “pine”, including:
- Amlodipine (Norvasc)
- Nicardipine (Cardene)
- Nifedipine (Procardia)
This type of CCB’s are more selective to peripheral vasculature than to cardiac cells, leading to arterial smooth muscle relaxation and decreased Systemic Vascular Resistance (SVR), thus, decreasing afterload and Myocardial Oxygen Demand (MVO2). Because of this peripheral calcium channel selectivity, they are commonly used for treatment of hypertension and angina.
Given their mechanism of action, patients and providers must be wary of potential adverse effects such as hypotension and reflex tachycardia secondary to decreased cardiac output.
Non-Dihydropyridine Calcium Channel Blockers
Non-dihydropyridines (DHPs) are CCBs that can be identified by a generic name not ending with “pine”, including:
- Diltiazem
- Verapamil
These are more selective to L-Type Calcium Channels in cardiac cells, slowing conduction across the SA and AV nodes which results in a negative chronotropic effect. This is useful for slowing rapid atrial arrhythmias such as atrial fibrillation or flutter with RVR.
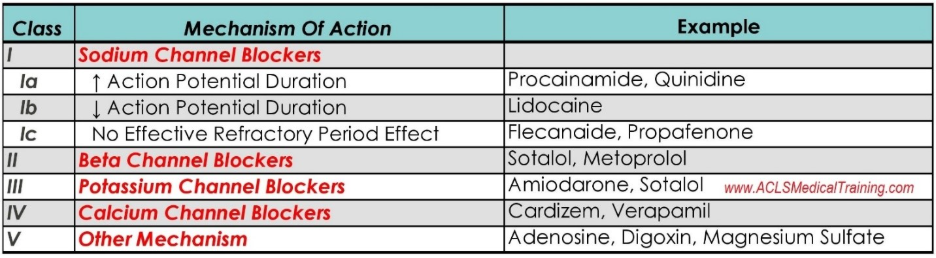
Vaughan-Williams Antiarrhythmic Classification System
The Vaughan-Williams Antiarrhythmic Classification System categorizes antiarrhythmic drugs into four primary classes with specific physiological functions based on their mechanism of action, with a fifth class later added to include “other” types.
Since each class works under a different mechanism of action, they have differing effects on cardiac cells. Some classes (II & IV) target SA and AV nodes and are primarily used for supraventricular arrhythmias such as AF with RVR or SVT. Others (I & III) target the His-Purkinje system and ventricular myocytes to manage rhythms such as ventricular tachycardia, while others have the capacity to address both atrial and ventricular arrhythmias. Diltiazem falls into the former category, as a Class IV antiarrhythmic, being used to treat atrial arrhythmias.
Indications for Diltiazem Use
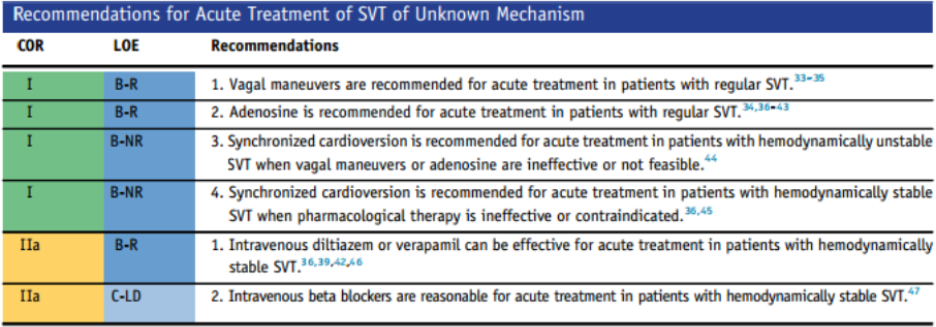
Guidelines from the American College of Cardiology and the American Heart Association give strong Class of Recommendation (COR) and Level of Evidence (LOE) ratings to the use of diltiazem in certain instances. Per the most recent guidelines (2023), diltiazem has a COR I, LOE b-r classification (strong recommendation / moderate evidence) when used for rate control of atrial arrhythmias, predominantly AF with RVR. Additionally, the 2015 guidelines still apply for diltiazem as a COR IIa, LOE-b classification (moderate recommendation / moderate evidence) for the treatment of SVT.
Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2024;83(22):2244–2356. doi:10.1016/j.jacc.2023.08.017
2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2015 Sep 16. pii: S0735-1097(15)06203-8. doi: 10.1016/j.jacc.2015.09.019.
Mechanism of Action of Diltiazem
Diltiazem produces three different “negative” effects on cardiac function via the blockage of L-type calcium channels:
- Chronotropic effect : The SA node’s pacemaker function slows its firing frequency (reducing heart rate).
- Dromotropic effect : The AV node slows its conduction velocity (assists in ventricular rate control).
- Inotropic effect : The myocytes decrease their force of contraction (reducing myocardial oxygen demand and ischemia).
When Diltiazem Should Be Avoided
Certain conditions can be dangerously exacerbated by the administration of diltiazem. These include pre-excited atrial fibrillation with Wolff-Parkinson-White syndrome with accessory pathways that bypass the regulation of the AV node. Since diltiazem further blocks AV node conduction, administration of the drug can lead to increased conduction through the unregulated accessory pathway, leading to life-threatening rapid ventricular rates. Instead of using diltiazem for these pre-excited arrythmias, alternative agents may be utilized including Procainamide and Ibutilide.
Diltiazem Use in Heart Failure and Hypotension
Given diltiazem’s negative inotropic effect, there are considerable risks for administering the drug to patients with reduced ejection fraction. Thus, diltiazem is generally avoided or used with extreme caution in patients with heart failure with reduced ejection fraction. Additionally, the drug is contraindicated in patients experiencing hypotension since the inotropic and chronotropic effects will exacerbate what is already a compromised cardiac output for the patient.
Dosing and Administration of Diltiazem
Per the most recent guidelines (2023), standard IV diltiazem dosing recommendations for rate control in patients with atrial fibrillation with RVR are as follows:
- 0.25 mg/kg over 2 minutes (15 to 20 mg)
- May repeat with a second dose of 0.35 mg/kg over 2 minutes (20 to 25 mg)
- Followed by a 5-15 mg/hr continuous infusion
Diltiazem as a continuous infusion can be titrated in increments of 2.5mg/hr every 15 to 30 minutes to maintain a goal heart rate of 80-100bpm. Patients should be monitored throughout infusion for signs of hypoperfusion or conduction abnormalities. BP should be taken every 5-15 minutes during bolus administration and titration, and continuous ECG monitoring performed to watch for PR prolongation or the development of AV blocks.
When Electrical Cardioversion is Required
It is crucial to remember that diltiazem is contraindicated in hemodynamically unstable patients with supraventricular tachyarrhythmias (whether atrial fibrillation or flutter with RVR or SVT). A patient is considered unstable if they are experiencing:
- Hypotension (SBP <90mmHg)
- Altered mental status
- Signs of shock (pale, cool, clammy skin, thready pulses or delayed cap refill)
- Ischemic chest pain
- Acute heart failure (pulmonary edema, shortness of breath, swelling, poor UOP)
Instead, treatment of hemodynamically unstable patients requires synchronized cardioversion at 120-200 J initially and should not be delayed for administration of an anti-arrhythmic agent.
Key Clinical Takeaways for Emergency Providers
In conclusion, diltiazem is a Class IV, non-dihydropyridine CCB anti-arrhythmic and is the most common pharmacological agent used for the treatment of atrial fibrillation and SVTs for patients that are hemodynamically stable.
It is critical that the patients’ cardiac rhythm be identified as supraventricular and that their hemodynamic status be ascertained prior to administration of diltiazem, since the decision for pharmacologic versus electrical intervention for tachyarrhythmias is dictated by these two factors.
In patients with new onset tachyarrhythmias, swift rhythm recognition and intervention are essential for positive patient outcomes. These skills are most effectively developed via exposure through ACLS courses and BLS courses which offer training for managing high stakes cardiac emergencies, empowering clinicians via certification courses. Visit our website to enroll today!
References
Antiperovitch P, Skanes A, Klein G, et al. Approach to a patient with asymptomatic pre-excitation. Heart. 2023;109(16):1254-1259. doi:10.1136/heartjnl-2022-321523
Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2024;83(22):2244-2356. doi:10.1016/j.jacc.2023.08.017
Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2016;67(13):1575-1623. doi:10.1016/j.jacc.2015.09.019
Sager PT, Kanter RJ. Calcium channel blockers in the treatment of cardiac arrhythmias. UpToDate. Updated October 24, 2023. Accessed March 11, 2026. https://www.uptodate.com/contents/calcium-channel-blockers-in-the-treatment-of-cardiac-arrhythmias



